






Worldwide, millions of patients are affected by dry eye disease (DED), also referred to as dry eye syndrome (DES). Many optometrists and ophthalmologists see patients with this condition regularly. In this article, we will outline the key elements to documentation, coding and claim completion.
Office Visit Coding
Monitoring early dry eye involves periodic office visits reported with the appropriate Evaluation & Management (E/M) (992xx) or eye exam code (920xx). The level of service depends on the severity and stability of the dry eye, what treatment is considered and whether other conditions are addressed at the same visit.
Diagnostic Testing
A variety of diagnostic tools can be employed to diagnose and assess DES and ocular surface disease, including patient questionnaires, lab tests and diagnostic tests. Not all are separately billable. See Table 1 below.
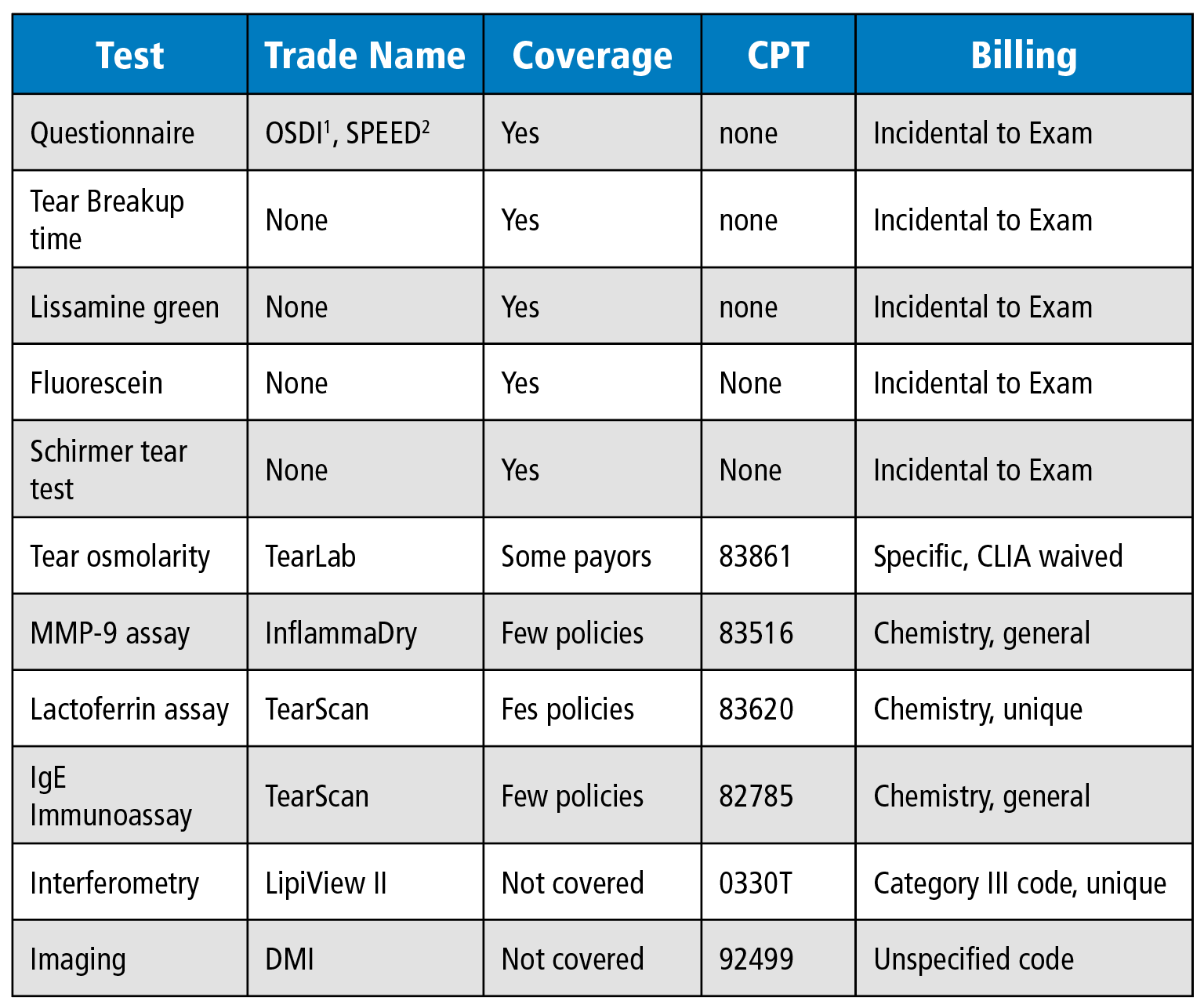
Don’t confuse coverage with separate payment. Covered services, even when not separately reimbursed, cannot be billed to the patient; non-covered services can.
Category III codes (T-codes) and miscellaneous codes (codes ending in 99) are not assigned relative value units and do not usually have predetermined reimbursement rates. This does not mean they are always noncovered. Since the 21st Century Cures Act of 2016 went into effect (in 2019), Medicare Administrative Contractors are prohibited from issuing a blanket non-coverage policies for all Category III codes. They must either issue an individual LCD for each code or make determinations on a claim-by-claim basis. Consequently, most providers must file claims unless the beneficiary instructs them not to.
Those involved with billing and reimbursement must check coverage and not assume the patient is financially responsible. Research might include inquiring with payors, reviewing recent policies, predetermining benefits and preauthorizing the service.
Communication and documentation are critical. Patients must be informed when coverage is uncertain. Document their understanding and acceptance of financial responsibility. For Medicare Part B patients use the Medicare ABN form. For all other payors, including Medicare Advantage Plans, use the Notice of Exclusion of Healthcare Benefits or a form provided by the payor.
Coverage
A variety of therapies are available for the millions of patients worldwide who seek care for dry eyes. The condition varies in severity between patients; no single therapy works for everyone. Medicare and other payers reimburse for reasonable and necessary services for the diagnosis, treatment or management of disease, injury and abnormalities. The type, intensity and timing of treatment option are important.
The phrase “reasonable and necessary” is defined and clarified in the Medicare Program Integrity Manual, Chapter 13 §13.5.4. It specifies “appropriate care” as care that “meets, but does not exceed, the patient’s medical need.” The order and timing of introducing various treatment options, may impact treatment. Step therapy, as outlined in DEWS II3 and DEWS III4, meets the patient’s need when introduced as part of the graduated treatment. This generally starts with artificial tears and lid hygiene and introducing punctal plugs or amnio tissue are introduced as needed, but not generally as the first line of treatment.
Intervention with minor surgery, punctal plugs or amnio tissue happens infrequently in the Medicare population. Based on data from CMS claims paid in 2022, optometrists inserted 9 punctal plugs (CPT 68761) for every 1,000 office visits (0.9%) and placed non-sutured amnio tissue (CPT 65778) twice for every 1,000 office visits (0.2%). For ophthalmologists, the frequency of use was 0.9% and 0.1%, respectively. Frequent use of the code or frequently repeated procedures on the same patients could attract payor attention.
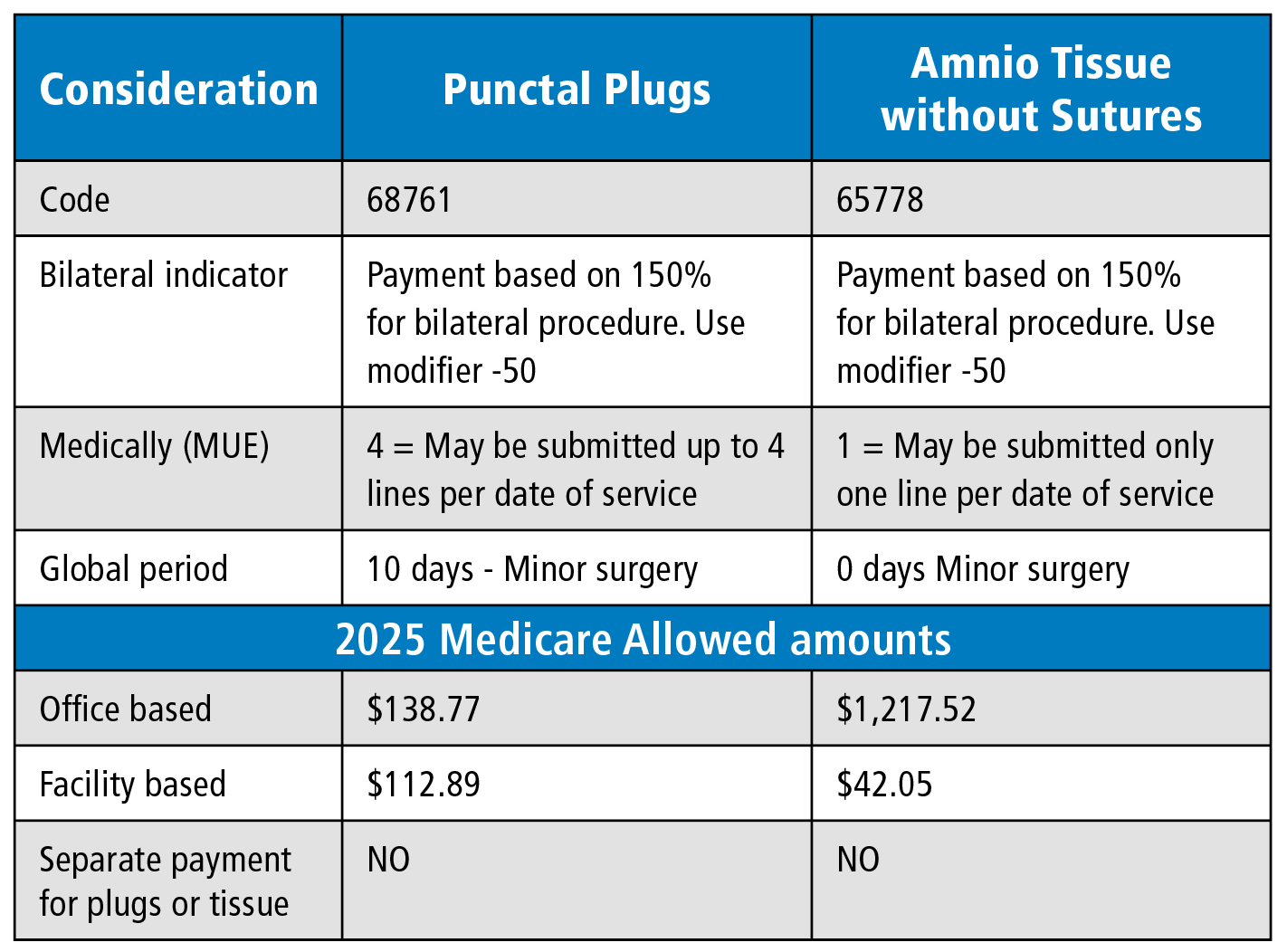
When billing for either punctal plugs or placement of amnio tissue for dry eyes, there are numerous coding considerations. Follow minor surgery billing rules related to the same day exam. A billable exam requires modifier -25.
Table 2
Conclusion
Providers and billers are encouraged to review their care patterns for DES management relative to the instructions in The DEWS studies and any payor policies available. Additionally, monitor claims for accuracy and timely payments. OP
References
1. Ocular Surface Disease Index (click here)
2. Standardized Patient Evaluation of Eye Dryness (SPEED) (click here)
3. TFOS DEWS II Report Executive Summary (click here)
4. TFOS DEWS III Report Executive Summary (click here)
